Our Location
Email Us
Phone Us
Cardiac Studies
Home / Cardiac Studies
Cardiac Studies
Heart disease is the leading cause of death for men, women of most racial and ethnic groups in the United States, the United Kingdom and in all developed countries around the world. More than 50% are heart attack and stroke.
According to Center for Disease Control USA (CDC) [1] and British Heart Foundation (BHF) [2] statistics:
• About 655,000 Americans die from heart disease each year—that’s 1 in every 4 deaths
• One person dies every 36 seconds in the USA from heart disease
• Heart and circulatory diseases cause around a quarter of all deaths in the UK; that's more than 160,000 deaths each year, or 460 each day – that’s one death every three minutes.
• (BHF) estimates that in the UK more than half of us will get a heart or circulatory condition in our lifetime.
• Around 4 million males and 3.6 million females are living with heart and circulatory diseases in the UK.
• About 18.2 million adults age 20 and older have coronary artery disease
• There are around 7.6 million people living with heart and circulatory diseases in the UK - an ageing and growing population and improved survival rates from heart and circulatory events could see these numbers rise still further.
• Around twice as many people are living with heart and circulatory diseases in the UK than with cancer and Alzheimer’s disease combined.
• Every year, 805,000 Americans have a heart attack
• Heart disease costs the US about $219 billion each year from 2014. This includes the cost of health care services, medicines, and lost productivity due to death.
• Healthcare costs relating to heart and circulatory diseases are estimated at £9 billion each year.
• CVD’s cost to the UK economy (including premature death, disability and informal costs) is estimated to be £19 billion each year.
Fibrinolytic therapy (FT) and Primary Percutaneous Coronary Intervention (P-PCI) are the two currently available modalities of reperfusion therapies. Both options are extensively studied. P-PCI decreases mortality and is superior to FT, especially if performed in a time at a high patient volume center [3]. However, there are many places in the world where immediate treatment of the ischemia, such as an invasive opening or bypassing of the occluded coronary artery is unavailable [4]. Delays in door-to-balloon times (D2B) are associated with increased mortality [ 5]. Although P-PCI is superior to FT, emphasis should be placed on timely administration of some form of reperfusion therapy rather than the mode of treatment. And such reperfusion that will allow to preserve and sustain the myocardium represent current unmet clinical need.
Besides direct heart muscle or brain tissue damage, cellular death with subsequent scar formation due to prolonged ischemia, massive cell damage with releasing of cell content in the extracellular space as well as hypoxia and cell hibernation predispose to reperfusion injury in such patients. The latter could potentially lead to life threatening arrythmias after myocardial infarction and to ischemia expansion, seizures, malignant cerebral edema, herniation, and other complications that significantly worsen clinical outcomes after stroke.
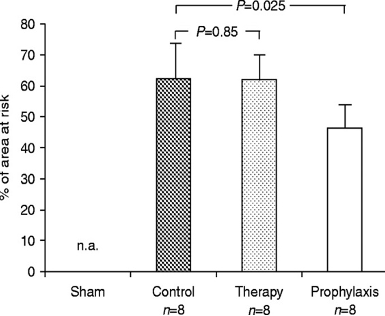
Previous investigations proofed the ability of one of the hemoglobin-based oxygen carriers (HBOC) to restore tissue oxygenation in long-term ischemia settings. HBOC-200, HBOC-201 and HBOC-301 were manufactured on the same facility using same patented technology. Small molecular size allows the material to achieve and oxygenate the remote regions where plasma but not RBCs may reach-in during severe occlusion of the artery, that supply this area. This is true for every organ and tissue in the body. And it is critical in the high oxygen demanding tissues such as heart muscle and the brain. There are studies specifically focused on the heart muscle oxygenation, including a randomized double-blind clinical trial that explored the comparability of the HBOC with blood in anemia settings after the open-heart surgery [6]. This study showed that the use of HBOC-201 eliminated the need for red blood cell transfusions in 34% of cases resulted in the similar discharged rate regardless hematocrit level in the HBOC group. Moreover, as well as the oxygen extraction was more significant in the HBOC group ( p< 0.05). Preclinical studies that used different protocols for ischemia prevention/treatment also showed benefits of the product derived from the bovine hemoglobin compared to no treatment or compared to other agents [7]. Thus infarct size in relation to the area at risk was significantly lower in the prophylaxis group than in the control group but no difference was seen after therapeutic application of HBOC-200. The size of the area at risk (percentage of left ventricle) was comparable between groups (control group, 30 (10)%; therapy group, 30 (10)%; prophylaxis group, 26 (7)%). The study concludes that neither prophylactic nor therapeutic application of the cell-free hemoglobin solution HBOC-200 aggravated cardiac I–R injury. Furthermore, the prophylactic approach may offer a new opportunity for pretreatment of patients at risk for perioperative ischemic cardiac events.
It’s well known that the heart consumes the highest amount of oxygen (O2) per tissue mass than any other organ and is exclusively dependent on aerobic metabolism to sustain adequate contraction. And any additional effort or the critical situation like stress, infection, anemia due to any cause increases myocardial O2 demand due to increased cardiac output as a compensation. In inadequate oxygen delivery to the heart the load increase can lead to the heart muscle ischemia and or dysfunction.
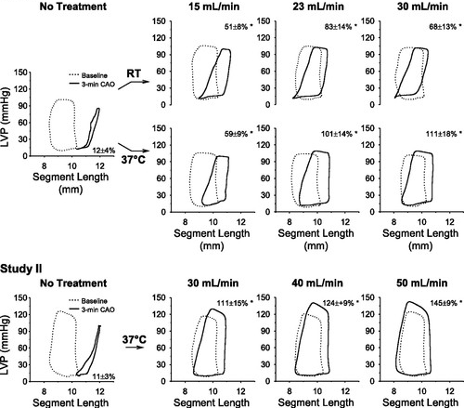
In study, performed by Te Lintel Hekkert and colleagues in 2010 [8], the effects of intracoronary infusions of preoxygenated HBOC-201 on regional myocardial oxygen delivery and utilization, global and regional LV function, coronary hemodynamics, and ventricular arrhythmias in a swine model of brief total coronary artery occlusions were investigated. The results of this study demonstrating myocardial protection with preoxygenated HBOC-201. This finding was a first and important step in exploring the efficacy of a pharmaco-invasive strategy using HBOC-201 in acute coronary syndromes and high-risk PCI. There have been claims by some that HBOC-201 and other HBOCs may have long-term detrimental effects, including an increase in the risk of myocardial infarction in patients undergoing major surgery or treatment of hemorrhagic shock [9, 10]. In contrast, Te Lintel Hekkert shawed that using repeated short-term intracoronary infusions resulted in cumulative systemic concentrations below 1 g%, did not reveal any adverse coronary or myocardial effects. Rather, full preservation by intracoronary preoxygenated HBOC-201 of myocardial aerobic metabolism and function in the absence of blood provides a profile of cardiac benefit and the absence of any intrinsic cardiac toxicity. One of this study objectives was to show the effects of preoxygenated HBOC-201 on regional myocardial segment length-left ventricular pressure relation responses to a 3-min CAO (Pic 2.) Hekkert’s findings allow us to speculate on the potential of preoxygenated HBOC-201 as an organ preservation fluid in the organ transplant setting. In conclusion, the present study demonstrates that intracoronary infusion of preoxygenated HBOC-201 during total CAO preserves regional myocardial contractile function and aerobic metabolism, by preserving myocardial oxygen delivery.
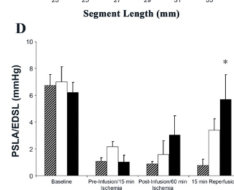
In another study in 2006 Isaac George e.a. [11] tested the impact of HBOC-201 on infarct size during acute and extensive (180 min) severe myocardial ischemia and reperfusion in gods. The researchers concluded that HBOC-201 usage improves regional myocardial function (Pic. 3) and reduces myocardial infarct size (Pic. 4) after acute coronary ischemia and reperfusion. Early and late administration of a bovine Hb solution after acute ischemia attenuates cardiac injury and increases tissue viability. The suggested further studies to investigate timing of administration and specific biochemical pathways to help clarify the optimal clinical use of HBOC-201 for treatment of acute myocardial ischemia.


Lee SK e.a. (2002) [12] tested the hypothesis that a small-volume bolus of HBOC-201 would improve and sustain brain tissue oxygen tension (PbrO2) without adverse effects on cardiovascular end-points, when used in an acute out-of-hospital hemorrhage model. In swine hemmorage model with mean arterial pressure (MAP) of 40 mm Hg standard hemodynamic parameters were monitored for 2 hours after the bolus infusion of hemoglobin oxygen carrier . In addition, Clark-type polarographic probes were directly inserted into brain tissue to measure PbrO2. Dr Lee’s group showed that the small-volume resuscitation with HBOC-201 rapidly restored hemodynamic parameters and PbrO2 following severe hemorrhage without detrimental vasoactive effects and without compromise to directly monitored brain tissue oxygenation (table 1).
Baseline | Hemorrhage | Oxygen | HBOC-201 | Observation | |
|---|---|---|---|---|---|
PbrO2 (mm Hg) | 25.7 ±: 1 | 6.9 ±: 5* | 14.8 ±: 12* | 42.6 ±: 4.8* | 40.9 ±: 9* |
CPP (mm Hg) | 75 ±: 11 | 32 ±: 4* | 32 ±: 6* | 49 ±: 8* | 77 ±: 13 |
PcvO2 (mm Hg) | 35 ±: 1 | 28 ±: 6* | 35 ±: 5 | 40 ±: 7 | 37 ±: 7 |
ScvO2 (%) | 66 ±: 3 | 45 ±: 16* | 59 ±: 9 | 72 ±: 5* | 66 ±: 7 |
AVDO2 (mL O2 /g Hgb) | 3.9 ±: 0.3 | 5.4 ±: 1.5* | Not measured | 2.8 ±: 0.6* | 3.2 ±: 0.7 |
John Caswell and colleagues [13] investigated the effects of HBOC-201 in a canine model of myocardial ischemia-reperfusion injury in 2005. They demonstrated that HBOC-201 has several positive attributes in the setting of MI/reperfusion injury.
A few important results were observed:
1. Cardiac damage markers were significantly lower in the group that received HBOC-201 – hemoglobin oxygen carrier, manufactured by Biopure Inc (Pic. 5,6,7).
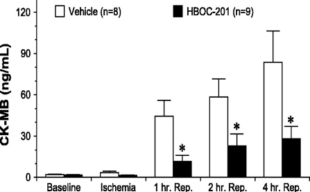
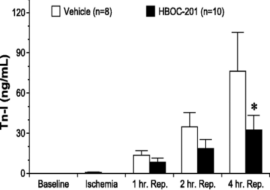
2. The myocardial infarct size was significantly decrease due to oxygen delivery restoration by the HBOC (Pic.8)
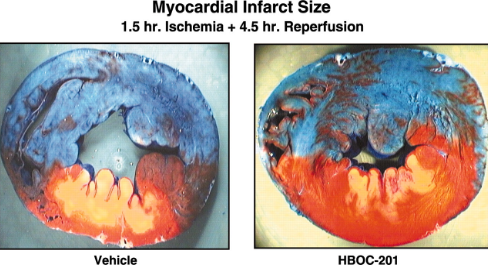
One limitation in the present study is that HBOC-201 was administered as a pretreatment, and this does not closely mimic what occurs during the evolution of acute myocardial infarction in humans. Another limitation is the short reperfusion time of 4.5 h. Additional studies to investigate 48–72 h of reperfusion will provide a better real-life analysis of the potential protective effects of HBOC-201. But this study clearly demonstrates that pretreatment with a Hboc-201 significantly ameliorates MI/Reperfusion injury. In addition, the extent of myocardial inflammation was also attenuated with this Hb-based blood-substitute therapy. Caswell also pointed out the need of additional studies to define the precise cellular and molecular mechanisms involved in this cardioprotective effect.
Cardioprotective interventions are needed before revascularization procedures to reduce adverse outcomes that result from the unavoidable delay between the onset of symptoms of an acute coronary event and revascularization. Ideally, patients experiencing atherothrombotic events should have access to cardioprotection before reaching the hospital. This currently is an unmet need. Hemoglobin based oxygen carriers, HBOC-201 in particular has been shown to increase myocardial oxygenation to provide an oxygen bridge until coronary perfusion is reestablished – this effect has been described by Daniel Burkhoff and coauthors [14] in 2005 who reviewed available literature that supports a cardioprotective effect for HBOCs administered in the setting of acute myocardial ischemia. According to this study “cardioprotective interventions are needed before revascularization procedures to reduce adverse outcomes that result from the unavoidable delay between the onset of symptoms of an acute coronary event and revascularization”. And this protection is needed on prehospital levels. And even though all these promising results were shown 15+ years ago such myocardial oxygenation bridge until coronary perfusion is reestablished remains an unmet medical need.
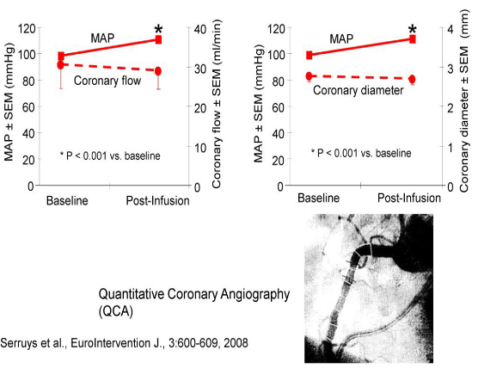
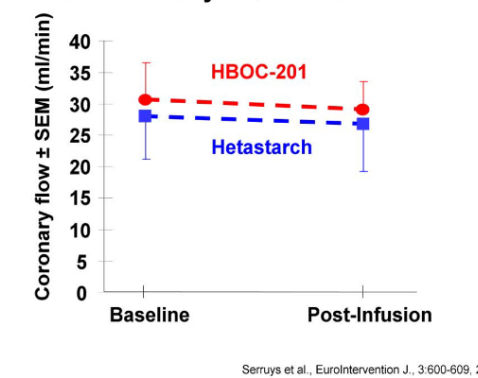
Human studies were conducted by Serruys and coauthors in 2008 [15] . Primary goal was to demonstrate the safety of the HBOC-201 regarding cardiac toxicity. Safety was proved by showing uncompromised coronary blood flow and preservation of LVSWI despite HBOC-201's known vasoactive effects. MAP rise were resolved with decrease of the infusion rate. Pic. 9, 10
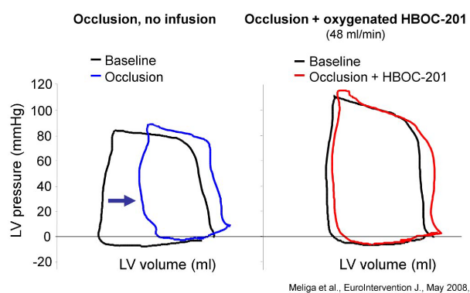
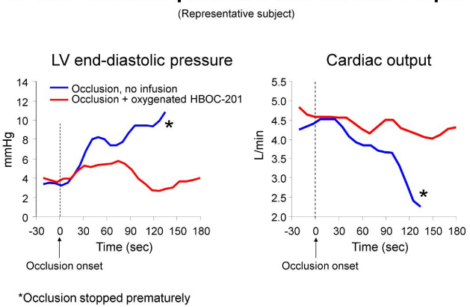
Subsequent study by Melinga et al. [16] showed that intracoronary infusion of oxygenated HBOC-201 can preserve left ventricular function, likely through maintenance of myocardial oxygenation. It is hypothesized, that in an acute setting, HBOC-201 could serve as an oxygen bridge to reperfusion by PCI extending the "golden" time period during which permanent myocardial damage is unlikely (Pic. 11, 12).
HBOC-201 of clinical trials in the treatment of ischemia
HBOC-201 may be useful in situations of critical tissue ischemia, locally such as in myocardial infarction (MI) and stroke or globally such as in traumatic hemorrhage, due to its ability to enhance convective and diffusive oxygen delivery to tissues compared to standard bloodless fluid therapies. By facilitating oxygen delivery in the face of common etiologies (thrombosis, embolism, trauma, intervention-induced arterial dissection) of acute ischemia, an oxygen therapeutic may also facilitate resolution of acute critical limb ischemia by promoting wound healing and preventing and/or reducing the incidence of re-amputation because of wound complications. Despite restoration of blood flow to ischemic tissues, persistent poor tissue perfusion secondary to microvascular pathologies may result in localized irreversible tissue damage. The rationale for using HBOC-201 in these indications is derived from the in vitro, in vivo, and clinical research conducted with this product.
Clinical trials (not published)
M9990-0075 A Multicenter, Double-Blind, Red Blood Cell-Controlled, Variable-Dose, Comparative Parallel Group Study to Evaluate the Effect on Allogeneic Blood Use and the Safety of Hemoglobin-Based Oxygen Carrier-201 (HBOC-201) When Administered in the Immediate Post-Cardiopulmonary Bypass Period, Universitaire Ziekenhuizen Katholieke Universiteit Leuven, Leuven, Belgium; Milpark Hospital, Parktown, Johannesburg, South Africa; University Hospital, Eppendorf, Hamburg, Germany. Phase II 1996 – 1997 Safety: All patients experienced at least one AE. The incidence of serious AEs, vital signs changes, lab abnormalities, EKG abnormalities and other safety findings were similar between treatment groups. Efficacy: A significant proportion of HBOC-201-treated, post-cardiovascular surgery patients (34%) received no transfusions of allogeneic RBC through the final follow-up visit (3 to 4 weeks). The mean number of units of RBC transfused was 1.54 in the HBOC-201 group vs. 2.17 in the RBC group. The median number of RBC units administered in the HBOC-201 group (1) was significantly (p=0.01) lower than in the RBC group (2).
COR-0001 A Multi-Center, Randomized, Double-blind, Placebo-controlled, Dose Finding Pilot Study to Evaluate the Safety and Feasibility of Hemoglobin-Based Oxygen Carrier-201 (HBOC-201) in Elective Percutaneous Coronary Revascularization for Subjects With Acute Coronary Syndromes. Erasmus Medical Center, Rotterdam, The Netherlands; University of Leipzig, Leipzig, Germany; Onze Lieve Vrouwe Gasthuis (OLVG) Amsterdam, The Netherlands; Academic Medical Center - Amsterdam, The Netherlands Phase II 2003 – 2005
Hemoglobin Based Oxygen Therapeutics in Elective Percutaneous Coronary Revascularization Erasmus Medical Center, Rotterdam, The Netherlands Phase II, 2007 Except for BP changes (which were corrected with the rate of infusion), there were no changes in other safety endpoints such as cardiac output, coronary blood flow, and pulmonary artery wedge pressure, and there were no cases of circulatory overload. In addition, laboratory assessment revealed no differences between groups in selected measurements of renal or liver function, cardiac biomarkers (CK-MB or cardiac troponin T), thrombosis, or inflammation.
BIOSA001 / BIOEU001 A Phase II, Multi-Center, Single-Blinded, Randomized, Placebo-Controlled Study to Evaluate the Safety and Feasibility of Hemoglobin-Based Oxygen Carrier-201 (HBOC-201, hemoglobin-glutamer-250 (bovine)]) on Wound Healing in Patients with Peripheral Vascular Disease and Who are Undergoing a Lower Limb Amputation due to Critical Lower Limb Ischemia Johannesburg Hospital, Johannesburg South Africa; John Radcliffe Hospital, Oxford, United Kingdom; Tygerburg Hospital, Tygerburg, South Africa Phase II, 2006 -2007
BIOEU003 “Enhancement of Tissue Preservation During Cardiopulmonary Bypass with Hemopure®” Phase II, 2006 – 2008 Thessaloniki Heart Institute, Milpark Hospital, Johannesburg, South Africa, Oxford Heart Centre - John Radcliffe Hospital, Headington, Oxfordshire, United Kingdom
References
For further information on OXY-Rx™ please contact us.
We would be happy to discuss it further.
0207 034 3300
We’d like to hear from you
Fitzrovia Hospital,
13-14 Fitzroy Square London, W1T 6AH
Please write to us
About
Markets
Contact